
|
Total body irradiation (TBI) remains an important component of conditioning regimens prior to hematopoietic stem cell transplantation (HSCT). Conventional TBI techniques are associated with significant toxicity and technical limitations. High precision volume modulated arc therapy (VMAT) such as RapidArc, provide improved target conformity and organ-at-risk (OAR) sparing. We report a dosimetric evaluation of two patients treated with linear accelerator (LINAC)-based RapidArc TBI as part of HSCT conditioning. Patient 1 underwent reduced-intensity conditioning (RIC) using single-fraction 4 Gy TBI, while Patient 2 received non-myeloablative conditioning (NMAC) with 2 Gy TBI. Treatment planning was performed using the Eclipse treatment planning system with multiple isocenters in head-first supine (HFS) and feet-first supine (FFS) positions. Both plans achieved satisfactory target coverage and dose homogeneity. In Patient 1, bilateral lung mean doses were 3.31 Gy and 3.26 Gy, with a conformity index (CI) of 0.96 and a homogeneity index (HI) of 1.09. The gamma index passing rate was 99.18%. In Patient 2, bilateral lung doses remained below 2 Gy, with gamma index passing rates above 98%. Organ-at-risk sparing and dose uniformity were successfully achieved in both patients. RapidArc-based TBI appears feasible, reproducible, and dosimetrically effective for HSCT conditioning, particularly in reduced-intensity and non-myeloablative transplant settings. |
Total body irradiation (TBI) continues to be a fundamental component of conditioning regimens prior to hematopoietic stem cell transplantation (HSCT) due to its established role in immunosuppression, eradication of residual malignant cells, and facilitation of donor stem cell engraftment [1,2]. Conventional TBI techniques using cobalt-60 teletherapy and extended source-to-surface distance arrangements are often associated with dose inhomogeneity, prolonged treatment duration, patient discomfort, and increased radiation exposure to organs at risk [2,3]. High-precision RapidArc techniques have demonstrated improved dose conformity, organ-at-risk sparing, and treatment delivery efficiency [4-6]. Additionally, reduced-intensity conditioning (RIC) and non-myeloablative conditioning (NMAC) regimens incorporating low-dose TBI have gained increasing acceptance for elderly and medically frail patients, as well as in haploidentical transplantation settings [7,8]. We report the implementation and dosimetric evaluation of LINAC-based RapidArc TBI in two patients undergoing HSCT conditioning using reduced-intensity and non-myeloablative approaches [4-6].
Two patients undergoing hematopoietic stem cell transplantation were selected for the LINAC-based RapidArc technique for total body irradiation after multidisciplinary evaluation involving radiation oncologists, hemato-oncologists, and transplant physicians. Both patients demonstrated adequate performance status and were considered suitable candidates for image-guided LINAC-based RapidArc technique TBI. Particular emphasis was placed on minimizing radiation exposure to critical organs at risk, including lungs, kidneys, and lenses, while maintaining satisfactory whole-body target coverage.
CT simulation was performed in head-first supine and feet-first supine positions using customized Vac-Lok immobilization to ensure reproducibility and patient stability. A 5-mm slice thickness scan was acquired with a 10-cm overlap region. The datasets were transferred to the Eclipse v17.0 treatment planning system, where the whole-body planning target volume (PTV) and organs at risk (lungs, kidneys, and lenses) were delineated. In patient 1, ovarian dose reduction was limited and could not be fully spared.
VMAT-based TBI planning was generated using the Analytical Anisotropic Algorithm (AAA v17.0.1) with 2.5 mm dose calculation grid spacing. Prior to treatment delivery, plan verification was performed using Varian EPID-based dosimetric quality assurance. Treatment was delivered on a VitalBeam® linear accelerator using 6 MV photons and image-guided radiotherapy (IGRT). Setup verification was performed prior to irradiation, and the patients successfully completed their regimens.
Patient1
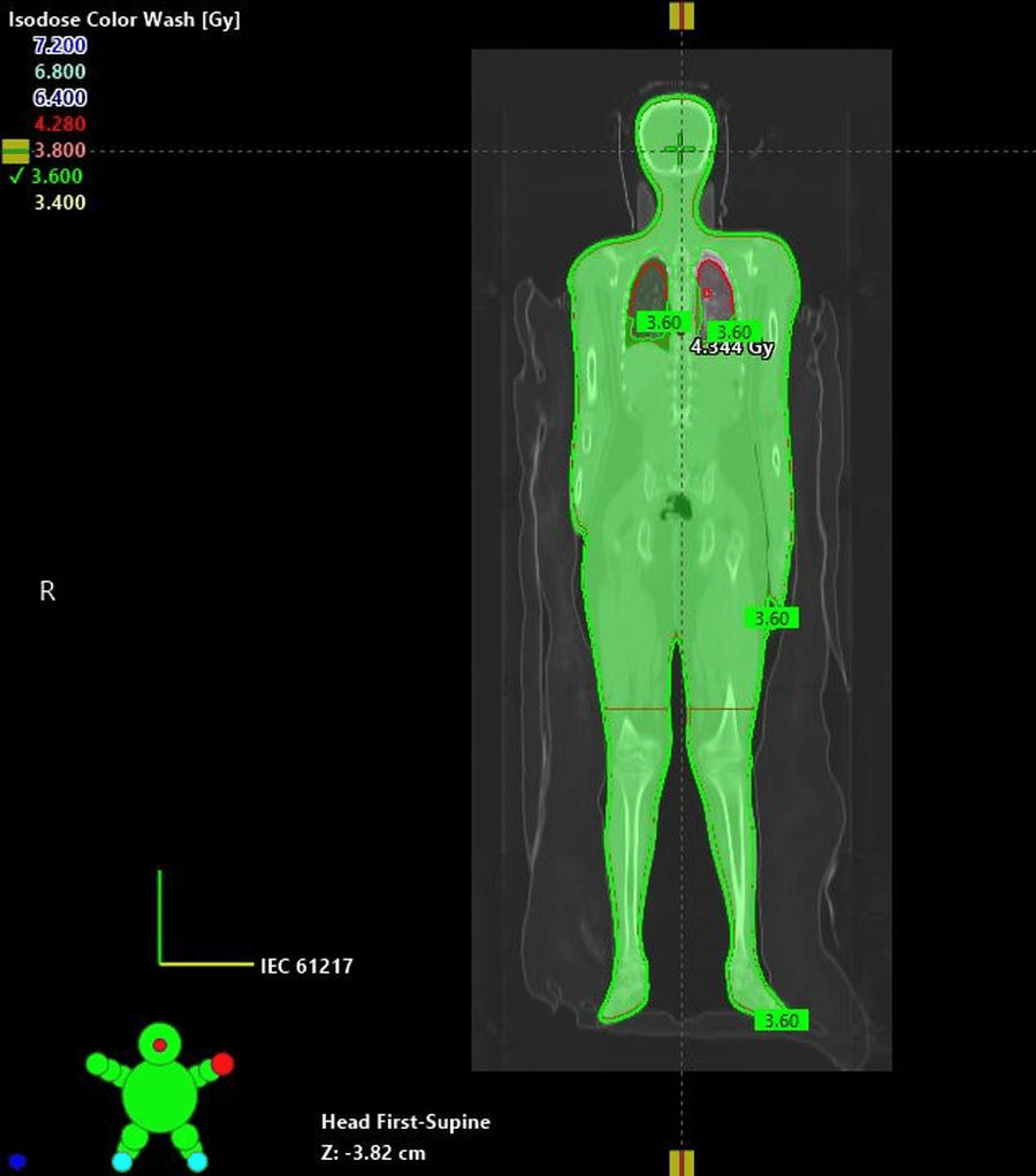
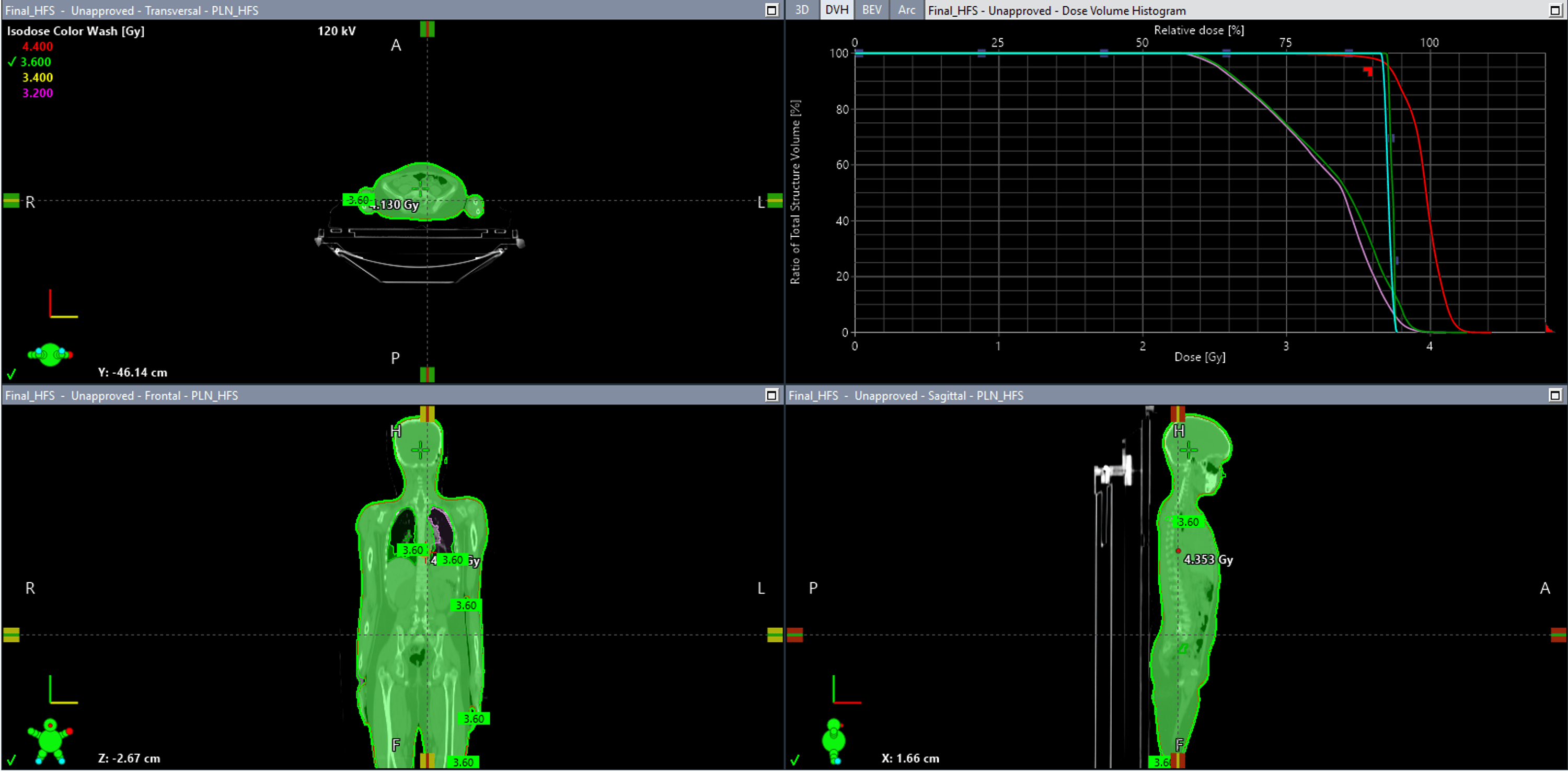
A 9-year-old female diagnosed with severe aplastic anemia underwent haploidentical HSCT with reduced-intensity conditioning incorporating single-fraction 4 Gy total body irradiation on day -1. The goal was to cover 90% of the target volume as shown in figure 1 while maintaining mean lung doses below 3.5 Gy. Treatment planning incorporated six isocenters, including four HFS and two FFS isocenters. The dose distribution and DVH (dose volume histogram) analysis of the RapidArc TBI plan are demonstrated in figure 2.
Dosimetric evaluation demonstrated in table 1, right and left lung mean doses of 3.31 Gy and 3.26 Gy, respectively. Mean kidney doses remained below 4 Gy bilaterally. The conformity index was 0.96, and the homogeneity index was 1.09. Gamma index analysis using 3%/3mm criteria demonstrated a passing rate of 99.18%, confirming accurate and reproducible dose delivery.
|
Parameter |
Value |
|
Right lung mean dose |
3.311 Gy |
|
Left lung mean dose |
3.266 Gy |
|
Right kidney mean dose |
3.959 Gy |
|
Left kidney mean dose |
3.947 Gy |
|
Right lens dose |
3.975 Gy |
|
Left lens dose |
4.027 Gy |
|
Right ovary dose |
3.770 Gy |
|
Left ovary dose |
3.764 Gy |
|
Maximum dose |
4.426 Gy |
|
Mean PTV dose |
3.952 Gy |
|
Gamma index passing rate |
99.18% |
|
Total monitor units |
3118 |
|
Beam-on time |
1740 seconds |
|
Homogeneity index |
1.097 |
|
Conformity index |
0.966 |
Table 1: Dosimetric parameters for patient 1
Figure 1: Coronal isodose color wash distribution demonstrating dose coverage achieved with VMAT-based total body irradiation (TBI) plan, showing satisfactory target dose homogeneity across the entire body contour.
Figure 2: Coronal, sagittal, and axial dose distribution with DVH analysis for RapidArc TBI planning.
Clinical Outcomes and Toxicity
Treatment delivery was well-tolerated with no acute intra-fraction complications. Following the conditioning regimen, Patient 1 experienced No acute parotitis, fatigue, or radiation-induced skin erythema was observed. Successful myeloid engraftment was achieved. At a current post-transplant follow-up of 4 months, the patient demonstrates stable donor chimerism with no clinical or radiological evidence of radiation pneumonitis.
Patient 2
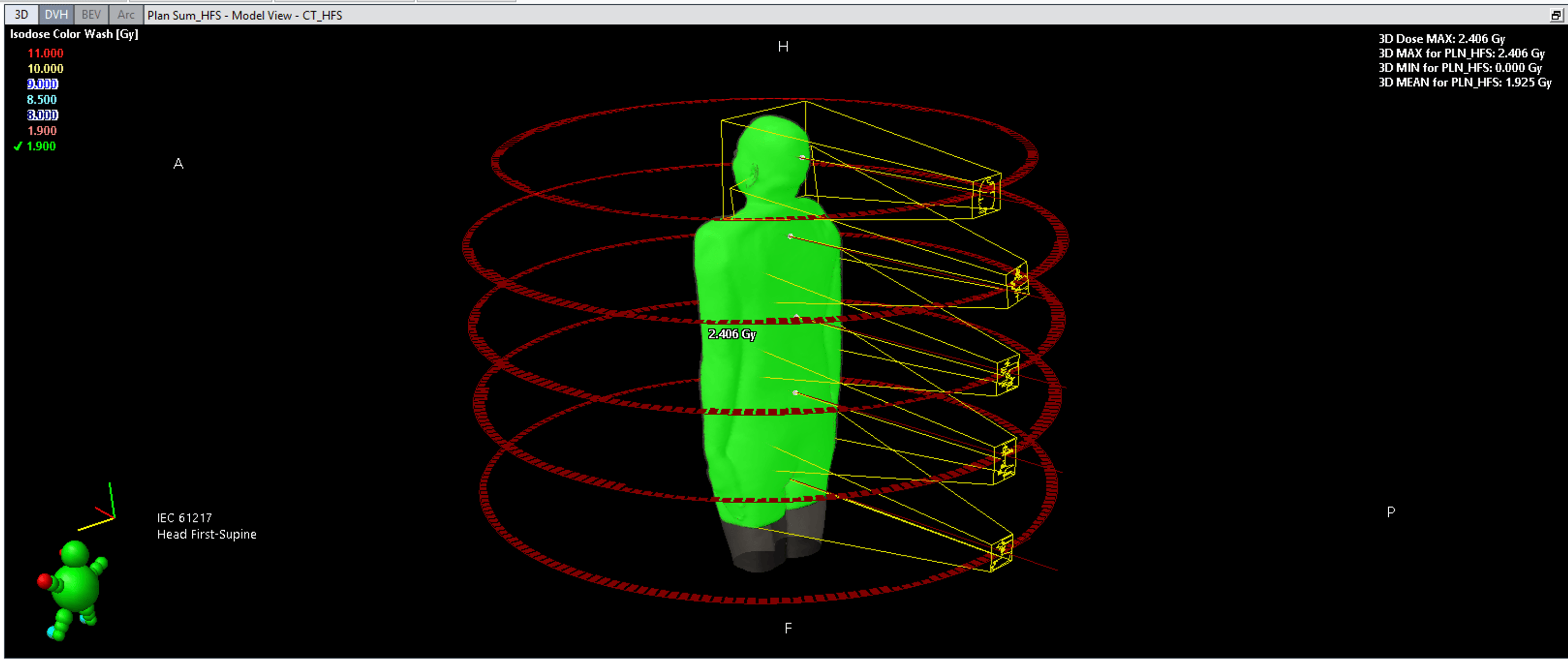
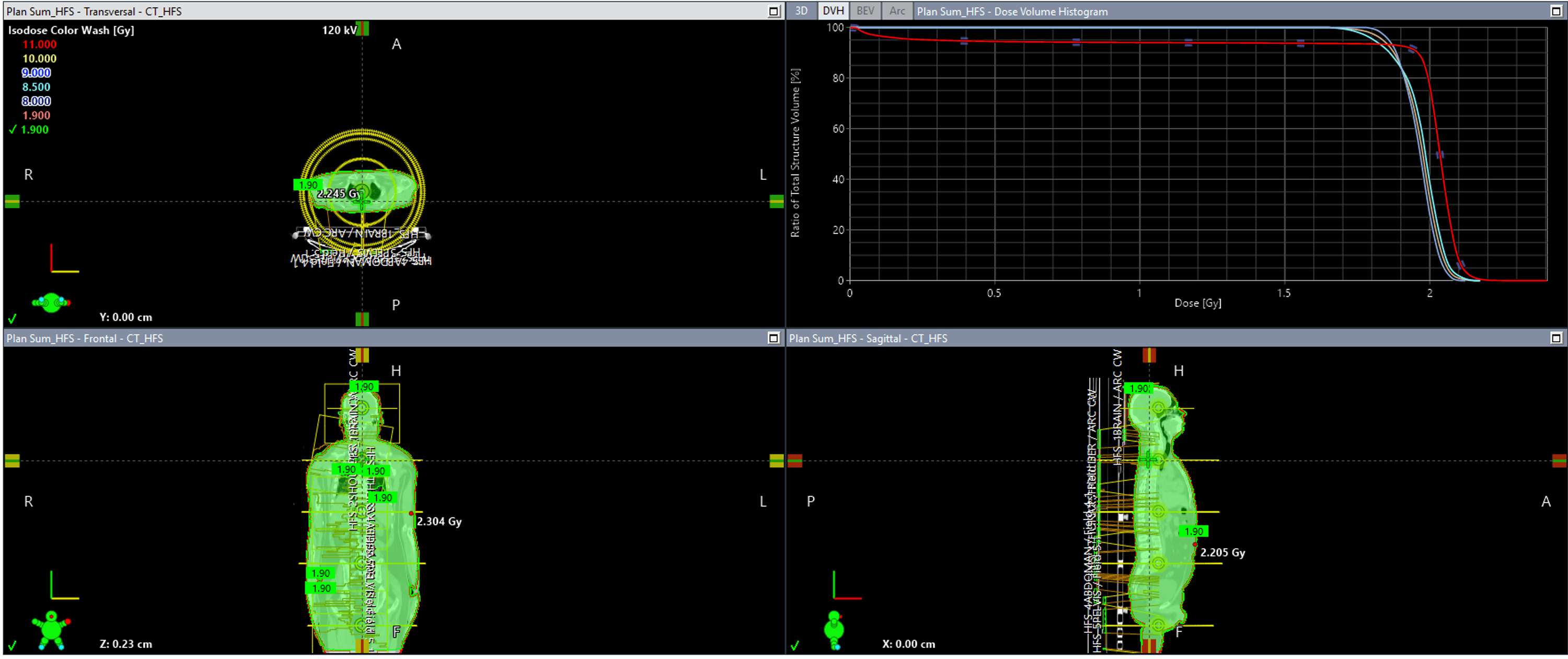
A 32-year-old male with chronic myelomonocytic leukemia and graft failure following a previous stem cell transplantation underwent a second haploidentical HSCT with non-myeloablative conditioning using single-fraction 2 Gy TBI. Case 2 utilized a total of 8 isocenters (four HFS and four FFS) with overlapping junctions to maintain dose homogeneity across the entire body as illustrated in figure 3.Bilateral lung doses remained below 2 Gy with satisfactory target coverage as shown in table 2. Gamma index analysis demonstrated passing rates above 98%, confirming reproducibility and agreement between planned and delivered dose distributions. Figure 4 presents the axial, coronal, and sagittal dose distributions along with cumulative DVH analysis for the prescribed 2 Gy VMAT-TBI treatment plan, showing adequate dose distribution.
|
Parameter |
Value |
|
Right lung mean dose |
1.97 Gy |
|
Left lung mean dose |
1.96 Gy |
|
HFS Dmax |
2.403 Gy |
|
FFS Dmax |
2.388 Gy |
|
HFS PTV mean dose |
2.042 Gy |
|
FFS PTV mean dose |
2.059 Gy |
|
HFS gamma index |
97.1% |
|
FFS gamma index |
99.6% |
|
Maximum point dose |
2.403 Gy |
|
Total monitor units |
2992.7 |
Table 2: Dosimetric parameters of the VMAT-based total body irradiation (TBI) treatment plan, including lung mean doses, PTV dose statistics, gamma index analysis, and total monitor units for head-first supine (HFS) and feet-first supine (FFS) setups.
Figure 3: Three-dimensional VMAT/RapidArc treatment plan demonstrating total body irradiation (TBI) dose distribution with multiple isocenters and arc arrangements in the head-first supine setup. The prescribed dose coverage and beam geometry are visualized in the 3D isodose model.
Figure 4: Four-window display of the head-first supine (HFS) VMAT-TBI treatment plan demonstrating axial, coronal, and sagittal dose distributions along with the cumulative dose–volume histogram (DVH), showing adequate target coverage and acceptable dose homogeneity for the prescribed 2 Gy fraction.
Clinical Outcomes and Toxicity
The single-fraction 2 Gy TBI regimen was exceptionally well-tolerated, with no acute gastrointestinal or constitutional symptoms noted during or immediately after irradiation. Given the patient's history of prior graft failure, close monitoring for secondary engraftment was performed. Sustained neutrophil engraftment (ANC>500/μl for 3 consecutive days) was documented on day +16 . During the acute post-transplant phase, the patient did not develop severe mucosal barrier breakdown or hepatic sinusoidal obstruction syndrome. At the last follow-up at 4 months post-transplantation, the patient remains clinically stable with no signs of late radiation-induced pulmonary or renal impairment.
TBI remains an integral component of HSCT conditioning regimens; however, conventional techniques are associated with substantial toxicity and technical limitations [1-3]. RapidArc technique-based approaches improve dose conformity and organ sparing while maintaining satisfactory target coverage [4-6]. In both patients, satisfactory dosimetric outcomes were achieved with acceptable organ-at-risk doses and reliable treatment delivery verification. Mean lung doses remained within clinically acceptable limits, potentially reducing pulmonary toxicity risk [1,2,6].
The excellent clinical tolerability observed in both patients directly mirrors the highly optimized dosimetric profiles achieved via RapidArc. By maintaining the mean bilateral lung doses well below the strict threshold of 4 Gy-specifically 3.31 Gy for Patient 1 and under 2 Gy for Patient 2-we effectively minimized the risk of fatal pulmonary toxicities such as idiopathic pneumonia syndrome (IPS). This clinical safety profile underscores the value of highly conformal RapidArc techniques over legacy 2D cobalt techniques, particularly when treating pediatric aplastic anemia or salvage graft-failure settings where tissue tolerance is heavily compromised [2,3,8].
Low-dose TBI has become increasingly important in reduced-intensity and non-myeloablative conditioning regimens [7,8]. Modern RapidArc technique-based approaches additionally provide opportunities for fertility preservation through reduction of gonadal dose exposure, although clinical limits must be recognised based on prescription constraints as seen in our pediatric cohort [9-11]. The limitations of this report include small sample size and lack of long-term clinical outcome data. Larger prospective studies are required to evaluate long-term toxicity and transplant outcomes.
RapidArc-based RapidArc technique total body irradiation is a feasible and effective approach for HSCT conditioning. The technique provides satisfactory target coverage, favorable dose homogeneity, and acceptable organ-at-risk sparing with reliable treatment delivery verification. RapidArc technique-based low-dose TBI may represent a promising strategy for reduced-intensity and non-myeloablative transplant conditioning protocols. In addition, the use of image-guided radiotherapy and multiple isocenter planning allowed accurate dose delivery across the entire body and good reproducibility during treatment. The dosimetric findings observed in both the patients suggest that VMAT-based TBI can be implemented safely while maintaining critical organ doses within acceptable limits. this approach may also improve treatment precision and patient comfort compared to conventional TBI techniques.

{kind=link}
{kind=link}
{kind=link}
{kind=link}